Teo thực quản
- Thứ tư - 15/11/2023 04:13
- In ra
- Đóng cửa sổ này
Teo thực quản
1. ĐẠI CƯƠNG
Teo thực quản ((Esophageal atresia)) là một dị tật hiếm gặp ở trẻ em trong đó thực quản bị gián đoạn có hoặc không kèm theo rò vào đường thở hay thực quản không gián đoạn mà thông với đường thở dạng chữ H, bệnh thường kèm theo nhiều dị tật khác. Tần suất gặp từ 1/2440 trẻ mới sinh tại Phần lan, 1/4500 trẻ mới sinh tại Úc và 2,82/10.000 tại Hoa Kì. Bệnh được William Durston mô tả lần đầu từ năm 1670 nhưng phải cho đến năm 1935 trường hợp teo thực quản không có rò khí quản đầu tiên mới được cứu sống bằng mở thông dạ dày và được nối thực quản khi bệnh nhân 11 tuổi. Trước năm 2005, TEO THỰC QUẢN được điều trị bằng phẫu thuật mở ngực qua màng phổi hoặc ngoài màng phổi. Năm 2002, Rothenberg và Bax đồng thời giới thiệu kỹ thuật mổ TEO THỰC QUẢN bằng phẫu thuật nội soi lồng ngực.2. NGUYÊN NHÂN
Không rõ ràng, có nhiều giả thuyết khác nhau về sự hình thành dị tật TEO THỰC QUẢN.3. CHẨN ĐOÁN
3.1. Lâm sàng
TEO THỰC QUẢN gồm có các thương tổn teo thực quản đơn thuần hay có rò với đường thở và tùy thuộc loại thương tổn mà có các triệu chứng đa dạng, trong đó có 86% biểu hiện thương tổn típ C với teo tịt đầu trên và thông đầu dưới thực quản với khí quản thường gây các triệu chứng:- Sặc khi cho ăn: ngay từ lần uống nước hoặc sữa đầu tiên trẻ đã bị sặc, nước hoặc sữa trào qua mũi, miệng.
- Trào nước bọt qua khóe mép: do nước bọt không được nuốt vào dạ dày được tích tụ ở đầu trên thực quản rồi trào qua khoang miệng ra ngoài.
- Bụng lép khi teo đầu dưới của thực quản không rò với khí quản. Bụng chướng trong teo thực quản có rò đầu dưới thực quản với khí quản.
- Không đặt được ống thông dạ dày.
3.2. Cận lâm sàng
Chụp X - quang lấy cả ngực và bụng, có bơm 1ml ba rít loãng vào đầu trên thực quản, để xác định vị trí đầu trên, tình trạng viêm phổi và bóng hơi dạ dày (Hình 1).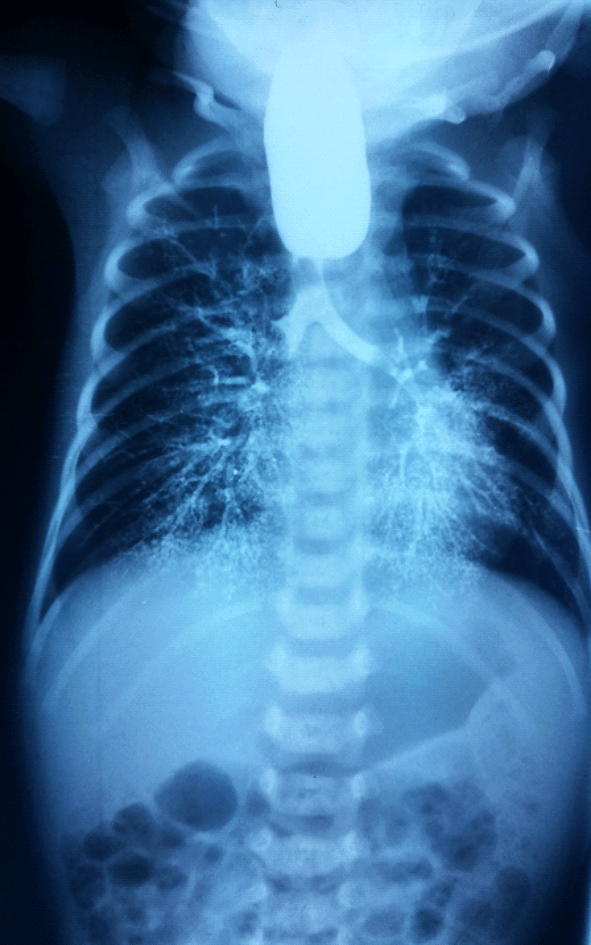
Hình 1.Hình chụp thực quản bệnh nhân TEO THỰC QUẢN có rò khí thực quản
Các phức hợp dị tật có TEO THỰC QUẢN:
- Phức hợp VACTER/VACTERL, Sparey thấy 10% các bệnh nhân teo thực quản bẩm sinh có phức hợp VACTERL.
- Phức hợp CHARGE: C = Coloboma of the eye: tật khe mắt, H = Heart defects: tật bẩm sinh tim, A = Atresia of the choanae: teo lỗ mũi sau, R = Retardation of growth: chậm phát triển, G = Genitourinary anormaly: dị tật sinh dục tiết niệu, E = Ear anomaly and/or deafness: dị tật tai và/hoặc điếc.Tiêu chuẩn chẩn đoán phức hợp CHARGE là cần có 4/6 dị tật được nêu trong phức hợp CHARGE.
3.3. Phân loại
- Phân loại theo tiên lượng: Dựa vào cân nặng, viêm phổi và dị tật tim phối hợp, Waterston 1962 chia TEO THỰC QUẢN thành ba nhóm A, B, C và khi có viêm phổi thì sẽ chuyển lên nhóm tiên lượng nặng hơn:+ Nhóm A: cân nặng > 2500g, không dị tật khác.
+ Nhóm B: cân nặng 1800g - 2500g, không dị tật khác.
+ Nhóm C: cân nặng < 1800g và có dị tật khác.
- Phân loại theo giải phẫu: Phân loại về TEO THỰC QUẢN dựa theo hình thái teo và liên quan với rò khí quản do Gross 1953 phân thành 5 típ, trong đó típ A chiếm 7%, típ B 1%, típ C 86%, típ D 2%, típ E 4%, típ F chưa thấy số liệu đề cập là tình trạng hẹp lòng thực quản.
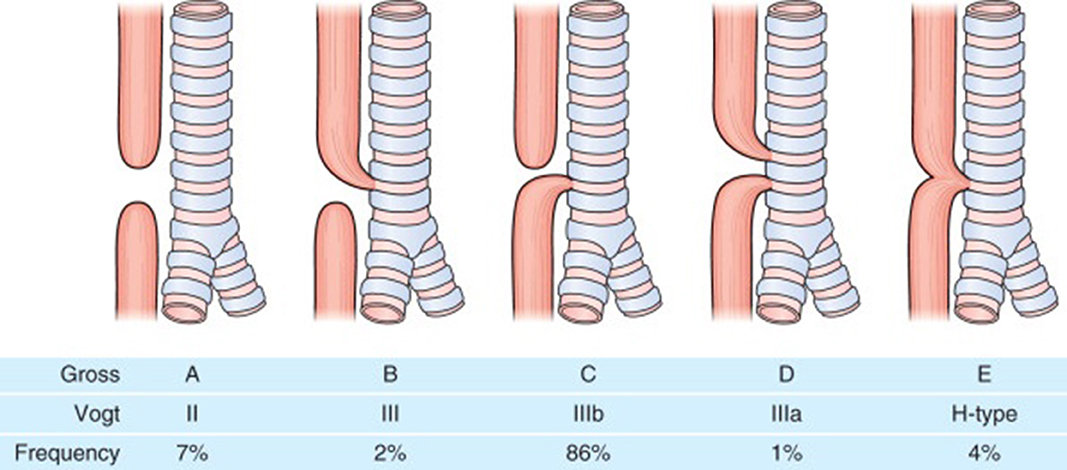
Hình 2.Phân loại các típ TEO THỰC QUẢN theo Gross (1953)
3.4. Chẩn đoán phân biệt
Dị tật khí thực quản, viêm phổi do các nguyên nhân khác, phân biệt với chụp cản quang thực quản, nội soi khí thực quản...4. ĐIỀU TRỊ
4.1. Mục tiêu, nguyên tắc điều trị
Cắt đường rò vào đường thở, lập lại lưu thông chức năng của thực quản.
4.2. Điều trị cụ thể
- Xử trí ban đầu:
+ Đặt bệnh nhân nằm đầu cao để tránh trào ngược dịch dạ dày qua lỗ rò thực quản khí quản vào phổi gây viêm phổi do hóa chất.
+ Đặt ống thông đầu trên, hút cách quãng dich ứ đọng.
+ Giữ ấm.
+ Siêu âm tim.
- Hồi sức trước mổ: Cho bệnh nhân thở oxy qua mặt nạ hoặc đặt ống nội khí quản nếu suy hô hấp nặng. Cần lưu ý không thông khí quá mức vì có nguy cơ làm dãn dạ dày do khí đi qua lỗ rò khí - thực quản.
+ Cấy dịch hầu họng trước khi dùng kháng sinh.
+ Duy trì thân nhiệt.
+ Điều chỉnh thăng bằng kiềm toan.
+ Bồi phụ nước điện giải.
+ Tiêm vitamin K.
4.3. Phẫu thuật mở chữa teo thực quản
- Tư thế bệnh nhân nằm nghiêng bên trái, có độn dưới ngực tương ứng.
- Mở ngực theo đường sau bên, qua gian sườn 3 - 4 bên phải.
- Bộc lộ khoang ngoài màng phổi.
- Đánh giá thương tổn đầu dưới, đầu trên.
- Cắt rời và khâu lỗ rò thực quản - khí quản.
- Nối hai đầu thực quản tận - tận, mũi rời.
- Một số kỹ thuật cho các trường hợp có hai đầu thực quản quá xa nhau:
+ Kỹ thuật nong dần đầu trên thực quản được Howard năm 1965 và Young tiếp tục phát triển năm 1967. Các tác giả dùng một ống thông đặt qua miệng vào đầu trên thực quản nong đầu trên thực quản hàng ngày hoặc 2 ngày 1 lần để đẩy đầu trên thực quản xuống thấp dần đến lúc có thể tiến hành khâu nối hai đầu thực quản với nhau (khoảng tuần thứ 6 - 12).
+ Kỹ thuật mở cơ đầu trên thực quản theo vòng tròn để làm dài thực quản được Livaditis đề xuất năm 1972.
+ Kỹ thuật tịnh tiến dần đầu trên thực quản được Ken Kimura thực hiện năm 1994. Trong kỹ thuật này, đầu trên thực quản được giải phóng và mở thông ra ngoài da cổ. Cứ 2 - 3 tuần, đầu trên thực quản lại được giải phóng và chuyển dần xuống thành ngực cho đến khi có thể nối được trực tiếp với dầu dưới.
+ Kỹ thuật khâu và kéo 2 đầu thực quản lại gần nhau trước khi nối hai đầu thực quản với nhau được Folker đề xuất năm 1997. Kỹ thuật được thực hiện bằng cách đặt nhiều mũi khâu vào 2 đầu thực quản. Các sợi chỉ khâu được để ở ngoài thành ngực và được kéo dần cho đến khi 2 đầu thực quản sát vào nhau.
4.4. Phẫu thuật nội soi trong điều trị TEO THỰC QUẢN
Năm 2002 Bax và Rothenberg cùng lúc đã công bố kết quả đầu tiên điều trị TEO THỰC QUẢN bằng nội soi lồng ngực.
4.5. Phương pháp tạo hình thay thế thực quản
Khi hai đầu thực quản quá xa nhau không thể nối trực tiếp hai đầu với nhau có thể tiến hành bằng dạ dày, đại tràng hay tiểu tràng thay thế thực quản.
5. TIẾN TRIỂN VÀ BIẾN CHỨNG
- Tỷ lệ thành công trong phẫu thuật điều trị TEO THỰC QUẢN đã không ngừng tăng cao theo thời gian. Theo Robert tỷ lệ tử vong vào năm 1955 là 33%. Tonz công bố tỷ lệ tử vong teo thực quản là 19,6% từ 1981 đến 1995. Tỷ lệ sống của teo thực quản tại Hà Lan báo cáo năm 2005 là 91%. Tỷ lệ sống theo báo cáo đa trung tâm tại Pháp năm 2013 là 95%. Tỷ lệ tử vong do teo thực quản tại các nước đang phát triển còn cao. Tỷ lệ tử vong tại Iran báo cáo năm 2012 là 56%, tại Malaysia năm 2013 là 23%.
- Biến chứng: hẹp miệng nối đến 50% cần được nong. Trào ngược dạ dày - thực quản có 47%. Rò khí - thực quản tái phát chiếm 10%. Mềm sụn khí quản chiếm 20%. Biến dạng lồng ngực....
6. DỰ PHÒNG
Chẩn đoán trước sinh để theo dõi, đánh giá sớm, dự phòng tình trạng nặng do viêm phổi và theo dõi tốt sau mổ.